

In clinical practice, many athletic patients I meet are naturally conscientious across several areas of life. They do not only train hard; they also tend to take work, studies, and other responsibilities seriously, often doing a great deal in all of them at once. When they come to the clinic, they may describe symptoms of exhaustion while also wondering whether they are “overtrained.”
This uncertainty is understandable. Burnout and overtraining syndrome can overlap in several ways: both may involve fatigue, declining performance, mood changes, impaired recovery, and difficulty tolerating stress. Yet the distinction matters. The ECSS/ACSM consensus report cites retrospective survey data in elite runners, in a discussion of NFOR/OTS risk, reporting that 60% of female and 64% of male runners indicated at least one previous episode of OTS during their careers [1]. The performance consequences, clinical meaning, and recovery timelines differ dramatically depending on where an athlete sits on this spectrum.
As both a doctor and former competitive athlete, I have seen this distinction matter in the consulting room and felt it in my own body. I wrote this article to help athletes, coaches, and clinicians think more clearly about whether burnout, functional overreaching, non-functional overreaching, or full overtraining syndrome may be dominant in a given situation, while recognizing that there is rarely a single easy answer.
The Spectrum: From Overreaching to Overtraining Syndrome
To understand burnout and OTS as distinct entities, it helps to first understand the training stress continuum. Successful training not only must involve overload but also must avoid the combination of excessive overload plus inadequate recovery [1].
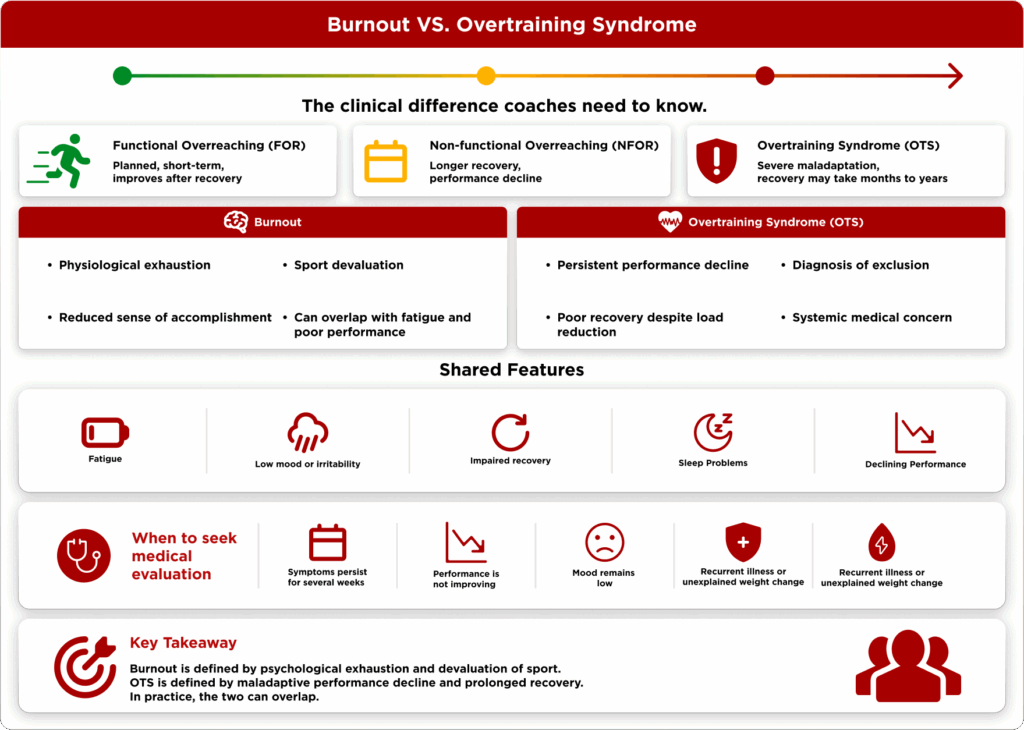
Functional overreaching (FOR) produces a short-term performance decrement without severe psychological or lasting other negative symptoms. This functional overreaching will eventually lead to an improvement in performance after recovery [1].
Non-functional overreaching (NFOR) produces a more prolonged performance decline requiring weeks to months for recovery. When athletes do not sufficiently respect the balance between training and recovery, NFOR can occur [1]. The distinction between NFOR and the Overtraining Syndrome (OTS) is very difficult and will depend on the clinical outcome and exclusion diagnosis. The athlete will often show the same clinical, hormonal, and other signs and symptoms [1].
Overtraining syndrome (OTS) represents the severe end of the continuum. It is characterized by sustained, unexplained performance degradation despite maintained or increased training volume, with recovery timelines ranging from months to years [1]. The difference between NFOR and OTS is based largely on time to recovery, not necessarily the degree or type of symptoms [1][2].
Functional overreaching can sometimes be a deliberate part of an athlete’s training plan. During my own competitive career, we would often place a period of functional overreaching early in the base-training phase. After that, with adequate recovery, supercompensation could raise conditioning to a higher level, and the goal was to time that peak so that fitness was at its best shortly before the main competition of the season.
The key point is that this was planned, monitored, and time-limited. It was not simply “training harder” for the sake of it. There were also times, however, when hard training was done without enough structure, guidance, or recovery. In those situations, the same basic idea could go wrong, leading toward non-functional overreaching, and at times, something much closer to overtraining syndrome.
I have experienced these states myself, and from that perspective I can say that true overtraining does not only affect performance. It can affect the athlete’s life more broadly: energy, mood, sleep, motivation, and the ability to function outside sport.
What Is Burnout — and How Is It Different?
Burnout is not simply a synonym for overtraining. Burnout is broadly defined as physical or mental exhaustion and a reduced sense of accomplishment that leads to devaluation of sport [4]. The three core dimensions are: (1) emotional and/or physical exhaustion; (2) reduced sense of accomplishment; and (3) devaluation of sport [4].
The critical differentiator is the third component. Sport devaluation — a negative attitude toward and psychological detachment from sport — is characteristic of burnout [4]. In contrast, OTS is primarily framed around maladaptive performance decline and systemic physiological disturbance. In practice, the two can overlap, particularly in athletes who also carry significant academic or professional stress.
Clinical reports describe OTS as being associated with decreased performance, increased injury and illness risk, and disturbances across endocrine, neurologic, cardiovascular, and psychological systems [4], making it clearly a medical concern, not merely a coaching one.
Many of the athletic patients I see who are at risk of overtraining are naturally hardworking and conscientious. In many ways, that is part of why they may end up in trouble in the first place. They are often capable of doing a great deal, but at some point the body can no longer keep up with the total load.
The same pattern often appears outside sport as well. These athletes may train hard, study hard, work hard, and carry significant responsibilities at the same time. Even when their general stress tolerance is good, the combined load can become too high. In real clinical practice, this is one reason burnout and overtraining syndrome may appear together, or at least look very similar at the bedside.
This overlap can make the distinction difficult. The athlete may not present with a clean textbook picture of either condition. Instead, the clinical question is often which process is dominant: psychological exhaustion and sport devaluation, physiological maladaptation to training load, or a combination of both.
The Hormonal Markers: What the Science Shows
One of the practical challenges for coaches is that there is no single blood test that diagnoses OTS. Because of the lack of a gold standard diagnostic test, OTS remains a diagnosis of exclusion [5]. However, understanding the hormonal pattern helps explain why an athlete’s performance collapses even when training loads appear manageable.
The most important finding from the research is also the most counterintuitive: basal hormone levels are mostly normal in athletes with OTS/FOR/NFOR compared with healthy athletes [3]. Relevant abnormalities may be more apparent during stimulation testing than in basal hormone measurements.
Stimulation tests, mainly performed in maximal exercise conditions, have shown blunted GH and ACTH responses in OTS/FOR/NFOR athletes, while cortisol and plasma catecholamine responses show conflicting findings [3]. Basal hormone levels are not good predictors, but blunted ACTH and GH responses to stimulation tests may serve as better predictors of OTS/FOR/NFOR [3].
From my perspective as a clinician, hormonal tests are usually less useful in real life than they may appear on paper. They do not confirm overtraining syndrome, and a single hormone panel often adds more confusion than clarity, especially when there are no healthy baseline values for comparison.
What I usually find more useful is a basic medical screen to rule out common causes of fatigue and poor performance. This typically means checking iron parameters, a complete blood count, and thyroid function at least once. These tests do not prove overtraining or burnout; they help ensure we are not missing something more straightforward, such as iron deficiency, anemia, infection-related changes, or thyroid disease.
Beyond excluding other medical causes, laboratory testing usually has limited value in distinguishing overtraining syndrome from burnout. The clinical story still matters more than any single number: training history, persistent performance decline, recovery pattern, symptoms, sleep, nutrition, life stress, mood, motivation, and whether the athlete has started to devalue the sport itself.
When a Tired Athlete Becomes a Medical Concern
The transition from a coaching concern to a medical concern occurs when performance decline persists despite adequate rest, when mood symptoms are sustained and worsening, when physical symptoms accumulate, or when the athlete expresses distress about their inability to recover.
Clinically, the diagnosis of overtraining syndrome remains one of exclusion, requiring the elimination of other potential causes including organic diseases, infections, negative energy balance, insufficient carbohydrate and/or protein intake, iron deficiency, and other medical contributors [1][5]. Medical evaluation is warranted when these features are present.
A physician approaching a potential OTS case will look to exclude other diagnoses before concluding OTS: endocrine disorders such as thyroid disease, iron deficiency with anemia, infectious illness, low energy availability or inadequate energy intake, disordered eating, and mental health contributors. Many of these are treatable, and identifying them early prevents unnecessary performance loss. Understanding cortisol and overtraining and the limits of standard hormonal testing is relevant to that clinical assessment.
Case series evidence illustrates the variable clinical trajectory: of three endurance athletes diagnosed with OTS, all showed typical OTS manifestations including impaired performance and multisystem dysfunction across endocrine, nervous, immune, and gastrointestinal systems, and two of the three successfully returned to competition following structured recovery [6].
As a practical rule of thumb, I would advise medical evaluation if an athlete has felt clearly unwell for several weeks, performance is not improving despite rest or load reduction, mood is persistently low, and there is a growing reluctance or loss of desire toward the sport. Everyone has good and bad days, and short periods of fatigue are part of training. But when the pattern lasts for weeks rather than days, something may be wrong — whether that is overtraining syndrome, burnout, low energy availability, iron deficiency, thyroid disease, infection, or another medical or psychological contributor.
In that situation, seeing a physician is not about “proving” overtraining with a single test. It is about stepping back, reviewing the whole clinical picture, and making sure that treatable causes are not being missed.
Conclusion
Burnout and overtraining syndrome can look similar from the outside: fatigue, declining performance, low mood, and poor recovery. Clinically, however, they are not the same problem. Burnout is marked by psychological exhaustion, reduced sense of accomplishment, and devaluation of sport, while overtraining syndrome sits at the severe end of the training-stress continuum.
For coaches and athletes, the practical message is not to label everything too quickly. Functional overreaching can be useful when it is planned, monitored, and followed by adequate recovery. But when fatigue persists for weeks, performance keeps falling, mood changes continue, or the athlete starts losing the desire to continue the sport, the situation deserves closer attention.
From my perspective as a doctor, the most important step is to look at the whole picture. Basic laboratory testing can help rule out treatable causes such as iron deficiency, anemia, infection-related changes, or thyroid disease, but normal bloodwork does not automatically exclude overtraining or burnout. The clinical story still matters most.
The earlier this distinction is recognized, the better the chance of preventing a temporary performance problem from becoming a prolonged medical and psychological setback.
About the Author
Dr. Antti Rintanen is a licensed medical doctor from Finland and a former athlete. He has a Master’s degree in Industrial Engineering and Management and a background in clinical medicine, orthopedic surgery research, and public health economics. As a former World Champion in Taekwon-Do and multiple-time World Cup titleholder in kickboxing, he combines medical expertise with first-hand experience of high-level training, recovery, and performance pressure. Through drantti.com, Dr. Rintanen writes evidence-based articles that help athletes, coaches, and clinicians interpret health, performance, and laboratory findings with more clinical context.
References
[1] https://pubmed.ncbi.nlm.nih.gov/23247672/
[2] https://pmc.ncbi.nlm.nih.gov/articles/PMC3435910/
[3] https://pmc.ncbi.nlm.nih.gov/articles/PMC5541747/
[4] https://pubmed.ncbi.nlm.nih.gov/38247370/

