Routine, something that most people wake up with and go to bed with, especially athletes. This will be a walk-through of monitoring and data collecting you need to carry out in order to keep your team, athletes and staff coordinated. I am a sports physio, and this will be my share of the knowledge of the most important aspects of sports.
Data recording
Initial testing is the starting point, the letter A in every preseason. Usually, this is your first encounter with the athlete. The ideal starting point is a conversation. A questioner that withholds all the questions you need in order to build an athlete profile. It starts simple, just a name and age, but then we get to the fun stuff.
Initial testing is the starting point, the letter A in every preseason.
Initial testing and diagnosis are done because everyone has locked potential. Some might expect athletes to always be at 100% readiness, but there can still be some hidden potential behind a deviation that stands out while you do a “reading” diagnosis of their body. It is very important to be conscious about your testing in the further steps so that you can differentiate various problems and help your athlete unlock all of their potential (3).
One of the most important questions is – What former injuries have you suffered?
This is crucial information! Find out as much information about it as possible – How it happened? Why has it happened? Is it a recurring injury? What was the therapy, how did it go and was it successful? These are just some of the most important questions one must do in the preliminary round of talks. The more you find out about the injury, the more likely it is that you will find correlating factors with some other injuries you have treated before. Gabbet in his article discusses the training-injury prevention paradox, which suggests that athletes who have a history of injury may need to modify their training programs in order to reduce their risk of future injury (4).
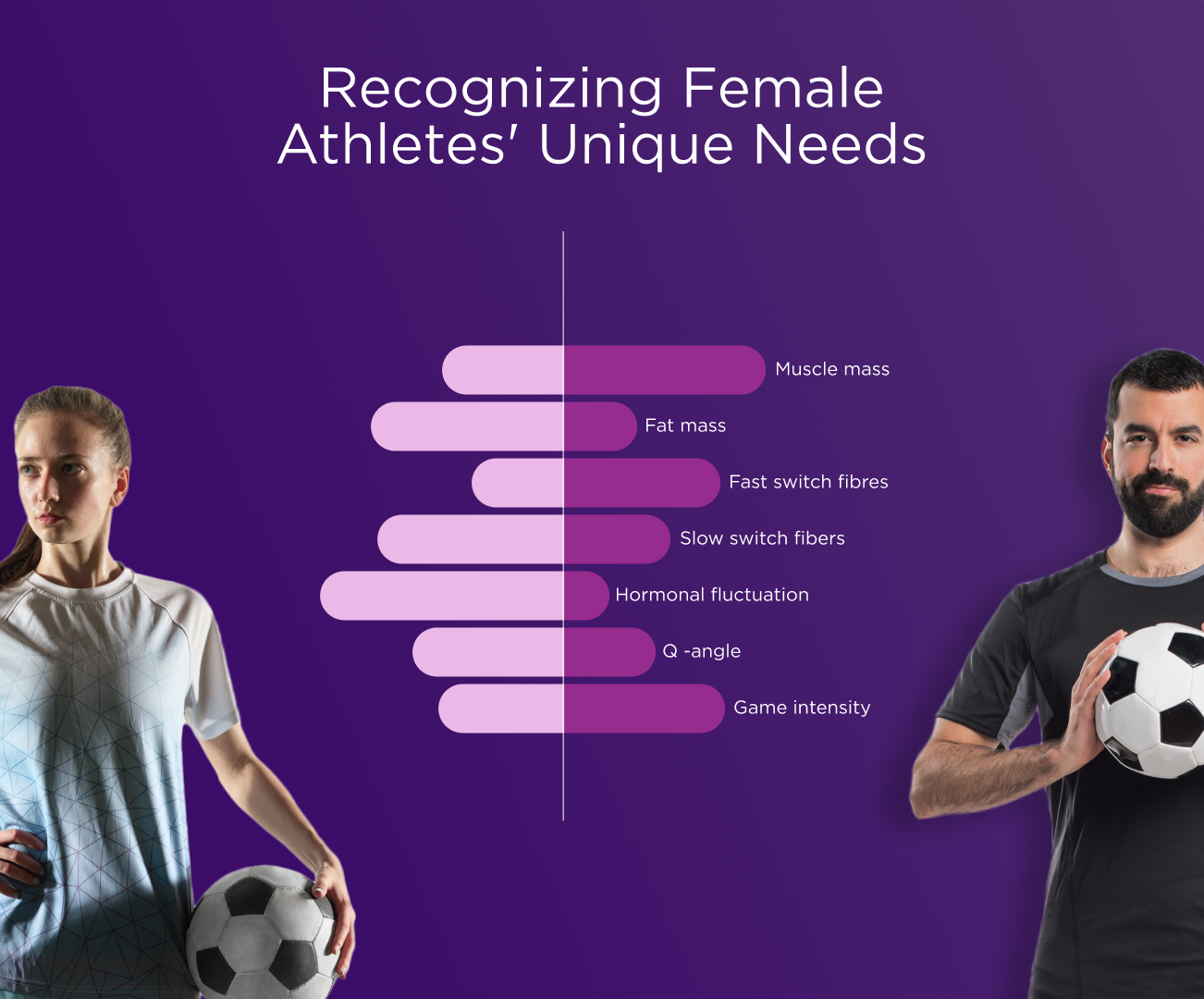
For instance, non-contact injuries are a direct indicator that a moment of adaptation did not occur. One of the most feared injuries for athletes, an ACL rupture can be solved surgically, but that might not eliminate the origin of the injury – lack of dorsiflexion, weak hamstring. There is a substantial body of research on the relationship between biomechanical factors and ACL injuries in athletes. Female basketball players with greater knee valgus (a movement pattern associated with ACL injuries) had reduced dorsiflexion range of motion compared to those with lesser knee valgus (1).
The more you find out about the injury, the more likely it is that you will find correlating factors with some other injuries you have treated before.
Functional testing can implement a range of specific tests for adaptation from the smallest joint, working their way all through the more general tests like FMS (overhead squat, leg raising, Thomas test, push-ups, rotary stability, lunging, hand reaching…).
One of my favorite specific tests, when it comes to kids and athletes preparing for a TEP hip surgery is the possibility of a foot to perform pronation and supination when needed. A person is standing straight and is rhythmically repeating rotations to one side. The same-sided foot should do a supination and the other foot should do a (hyper) pronation. A more general test, that everyone has probably heard of, is the single leg hop test. Generating the force dominantly out of the leg, the whole body will give you information about the ROM, stability, and motor control.
Fitness tests are more suited for strength & condition coaches, but they also require the full attention of a physio. Fitness is a huge risk factor for potential injuries. Something that needs to be brought up in the conversation between the head coach, S&C, and the physio is the aspect of motor control. Quality of movement is a very subjective aspect and is sometimes impossible to grade objectively.
So, if you do find something suspicious get into it from all aspects. Check the results of the previous tests, here you can notice red flags as serious as cardio-respiratory problems (loss of breath, chest pain) or soreness distribution during the testing.
On-the-field testing : Day to day
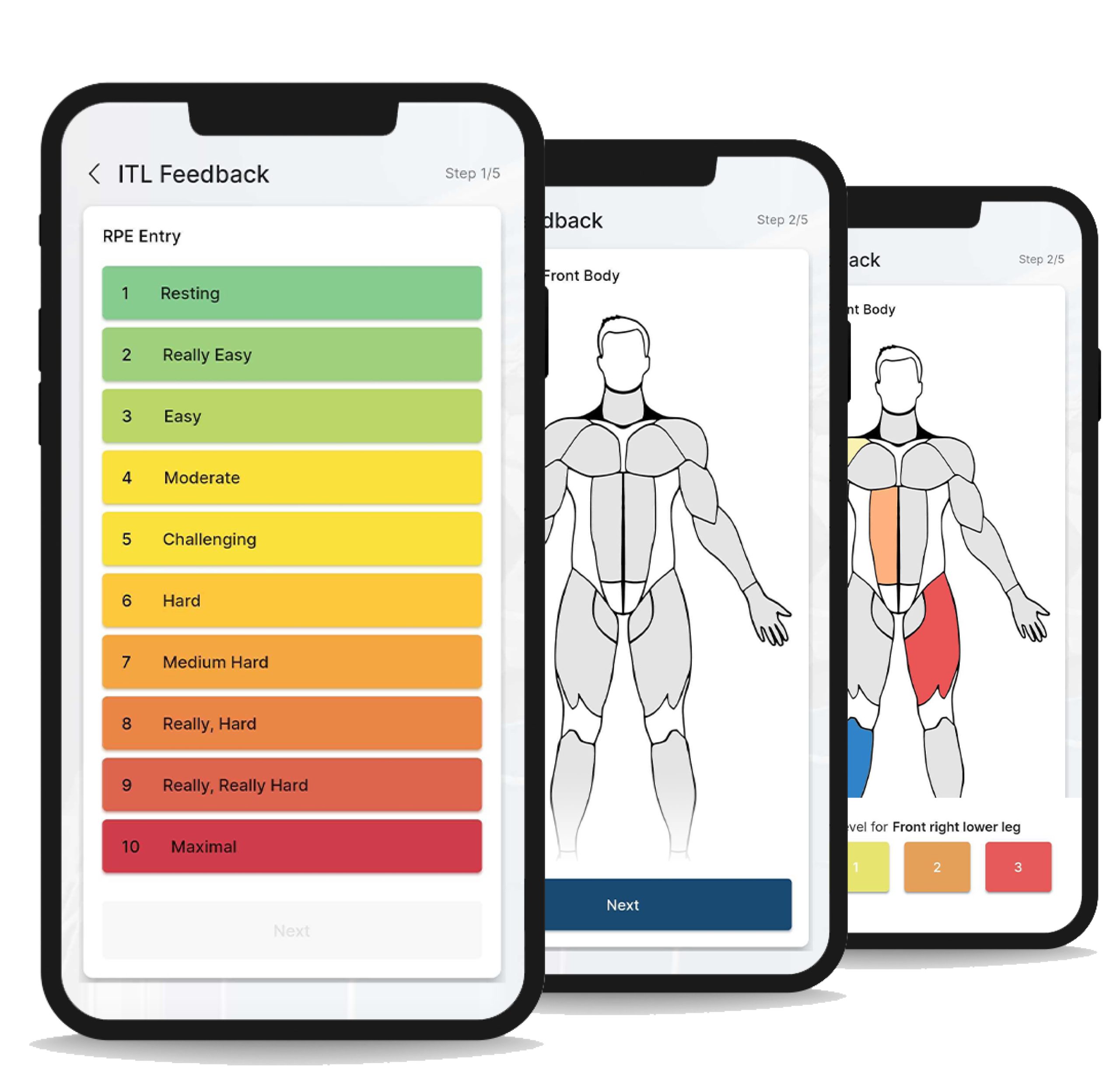
When you work in team sports, your tools must be efficient, easily explained to the athletes, and practical in order to gather data. After the initial testing, you will have a clearer picture of the athletes you are working with. The next step is to differentiate individuals in the team and have specific approaches for each one of them. This is where day-to-day monitoring becomes one of the most crucial parts. You have to watchfully monitor your athletes about their current state and keep an eye out for possible red flags that could lead to future injury. My recommendation would be an RPE scale and a picture chart. Usually, the simplest methods turn out to be the best!
RPE scale has proven to be one of the most useful tools not only in my practice but also for the athletes themselves. Through it, they get to know themselves and how to grade their own levels and perceptions of fatigue. The use of it is also extremely simple, rating your level of fatigue on a 1-10 numeric scale.

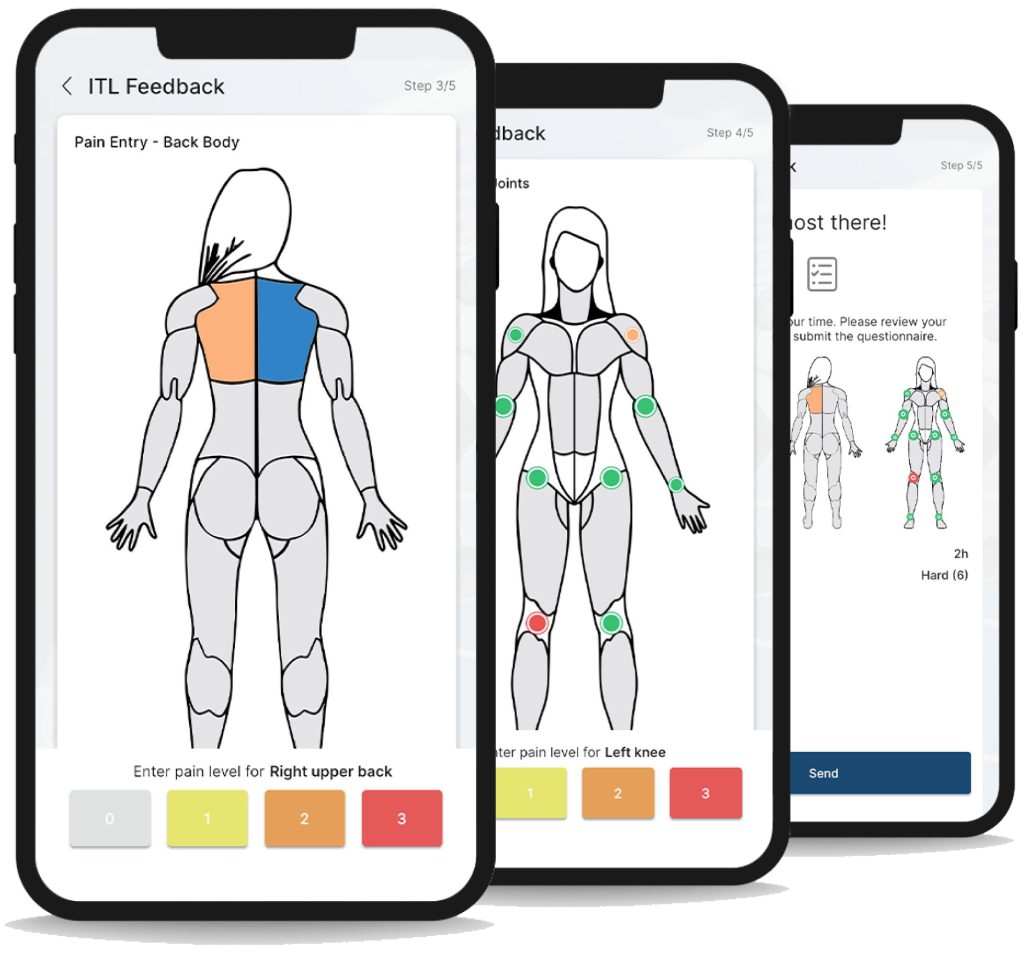
Picture chart is of equal importance. Signalizing their pain, ace, soreness, or scratch. It is of extreme importance that athletes learn to verbalize/vocalize their problem – the area that is affected, the movement which is causing it, the timing, and the kind of pain.
Always be on alert/present
Sometimes a problem can go under the radar and won’t show until a session starts. Those are the ones you must look out for. Athletes sometimes believe that a certain problem is not important enough for them to mention it – they can just walk it off. That is why one of your most important jobs is to be present and observe them on the field. It is not uncommon that the first few steps and mobility drills show indications of a problem. If you notice problems during the warm-up session those players should be taken off the court immediately. During the training session, strength and conditioning part should not be of any trouble. Proper form and skilled strength and conditioning coaching should keep you calm and aligned with your goals for each athlete. Specific training is usually where the trouble starts, long shots and contact can easily lead to injuries. But if you have done all the preparation correctly, without skipping any steps, there should not be any surprises.
Seal the deal
No matter the age, gender, or level of competition you will work with individuals who already have a history of their own with sports, injuries, and life itself. You have to respect each individual, look into their past, and observe who they are now (from the postural organization to functional and fitness tests), all in order to help them become the best version of themselves. The real challenge and indicator of skill is the day-to-day monitoring, which tracks the wellbeing of your players and your work with them as well. The way you gather and interpret the information will greatly affect the course of an athlete’s performance and will be mirrored on the field and in the end result.
References:
- Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003 Oct;35(10):1745-50.
- Leppänen M, Pasanen K, Kujala UM, Vasankari T, Kannus P, Äyrämö S, Krosshaug T, Bahr R, Avela J, Perttunen J, Parkkari J. Stiff Landings Are Associated With Increased ACL Injury Risk in Young Female Basketball and Floorball Players. Am J Sports Med. 2017 Feb;45(2):386-393.
- Gabbett TJ. The development and application of an injury prediction model for noncontact, soft-tissue injuries in elite collision sport athletes. J Strength Cond Res. 2010 Oct;24(10):2593-603.
- Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. 2016 Mar;50(5):273-80.