We do what we can
A few years ago, I attended a Strength and conditioning conference where during a lecture, one S&C coach said: „There is no such thing as injury prevention – only injury reduction “- and that cannot be truer. We can only do so much to help athletes, and we can’t prevent injuries 100%. This takes us to – rehabilitation. It’s important to emphasize that we cannot look at rehabilitation as a separate field anymore. Today, it is inevitably connected to S&C, load management, programming, and other complex areas of sports science and physiotherapy. Physiotherapists do not operate alone, so multidisciplinary expertise is a must-have. Load management, monitoring, strength training, periodization, RPE, etc. – are all important factors in rehabilitation today and to understand our job requirements, we need to get to the base of them.
Why is it important to know these terms – because working with athletes requires working in team surroundings and proper communication with other team members is crucial – S&C coaches, head coaches, football coaches, basketball coaches, and data scientists. Some aspects will require less and some more detailed knowledge, but we must understand the basics. So, if we are talking about rehabilitation pillars, I would first start with – communication.
„There is no such thing as injury prevention – only injury reduction.“
Communication
With communication comes psychological assessment. Here we are referring to a general personality assessment. There are usually two types of athlete personalities regarding the return to the sport decision-making process. Type A – the overcautious athlete. This type will require more reassurance and encouragement to start training with the team. Type B – is the overconfident athlete. This type is the opposite, they will want to return to their training schedules sooner than they should, in such cases, you need to slow them down, make them wait, and work on their patience. Of course, not everything is black and white and you have to approach every athlete individually, but if you were to imagine a scale from 1 to 10, 1 being the overcautious athlete and 10 being the over-confident athlete, you can choose a number for each athlete as you get to know them. According to the number on the scale, choose the right approach strategy.
Setting expectations
Today we have a big database of match and training injury rate in relation to absence from training (in days) by UEFA and other institutions that gather their info on a vast number of athletes. So, if an adductor grade 2 injury on average takes 18 days before return to sport (1), that can be a good way of communicating expectations to the athlete, of course, after emotions settle down and when the athlete is calm enough to hear the prognosis. Informing them immediately after the injury takes place while still feeling emotional can be overwhelming for some, if not for most of them.
Rehabilitation Milestones
Regarding rehabilitation, a milestone would be a specific stage during return to sport rehabilitation. Range of motion (ROM) strength tests, endurance tests, pain scales, and specific movement or orthopedic tests can all be considered milestones in this case. By setting clear milestones in the beginning and through open communication with the athlete, the risk of a recurring injury can be decreased by 60%. The athlete will be able to set clear goals for themselves and also openly communicate if there is pain throughout the rehabilitation process. Better communication leads to increased effectiveness and a successful return to sport protocol.
The most important milestone is the last one, which the athlete needs to accomplish before returning to play so we should be most meticulous in setting that one. Why? Because the athlete is eager to play as soon as possible, and again, needs to have realistic expectations when he is able to play with minimal injury risk. For example, with an adductor strain, we need to have a completely pain-free athlete before returning to training with the rest of the team. Of course, each milestone depends on the nature of the injury, so the number and type of milestones can differ from athlete to athlete, and injury to injury.
Setting load in rehabilitation
How to set load for a rehabilitation exercise? Percentage (%) of 1 RM, RPE, RIR? So, a 1 RM (when talking about strength) would be the most or maximum amount you can lift in one repetition. For example, when implementing a muscle hypertrophy program for the athlete, we can use 60-80% of 1RM and perform 8-12 reps of an exercise. Honestly, in my environment, I rarely used % of 1 RM during rehabilitation. Although, I must say the biggest reason was that the work conditions didn’t allow it. But I don’t think I lost much with it, because I find RPE (rate of perceived exertion) and RIR (reps in reserve) a really good method for measuring exercise intensity – under one condition – that the athlete is well educated about the method. With rehabilitation, there is of course – the pain component. So, we will use the NRS (numerical rating scale) in cooperation with RPE or RIR to determine how hard we will train i.e., to determine the training volume. So, how do the methods work?
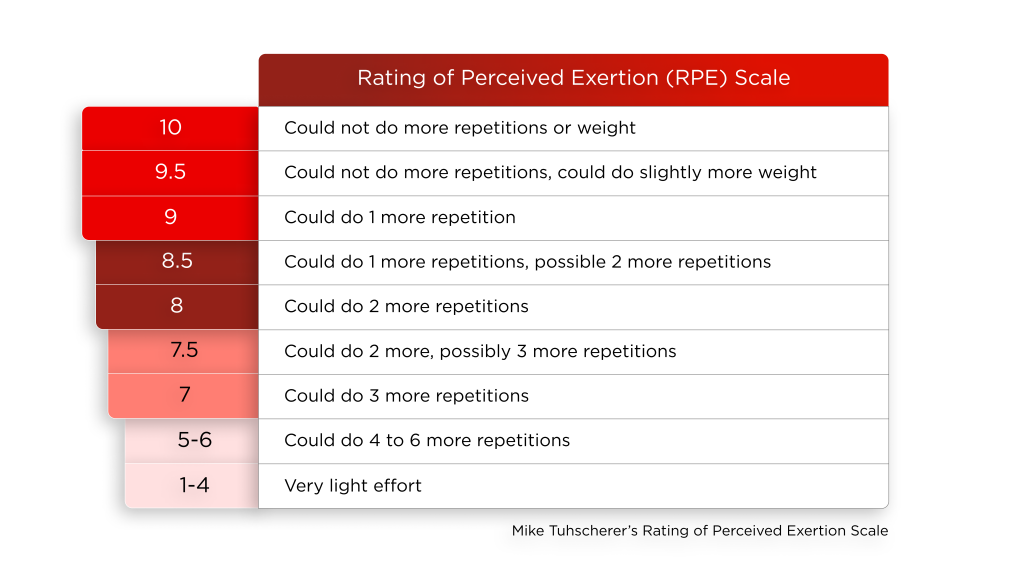
Rate of perceived exertion
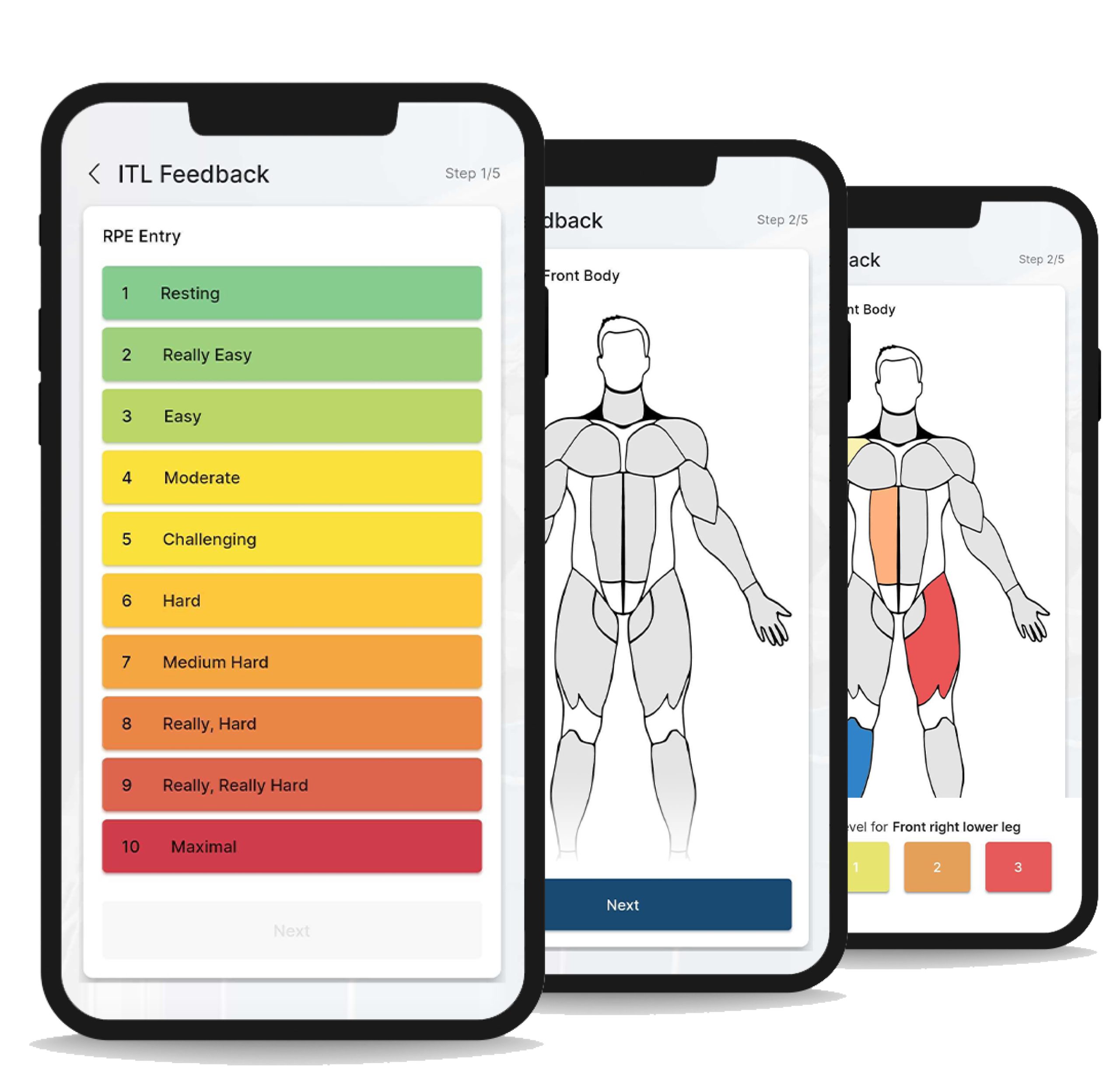
RPE functions on a scale of 0-10, with 10 being the highest intensity value, and 0 being the lowest. (Table below) It’s basically a subjective measure of how hard you train. Depending on the specificity of the injury, we might have different goals during different phases of the rehabilitation process. Let’s say we have an adductor strain and we are doing core stability exercises that are completely pain-free for the athlete. Here, one should start with a high RPE value from the very beginning, in order to improve core stability as much as possible in the limited amount of time available. So, a 7 or even an 8 would be the number of choice.
NRS – Numerical rating scale
What if our athlete experiences pain during an exercise? The answer, of course, depends on the nature of the injury and the nature of the exercise. The NRS is, again, a subjective measure of pain intensity. The scale is from 0-10, where 0 represents no pain at all, and 10 would be maximal pain intensity a person can feel. This is where getting to know your player personality becomes very important. Different personalities will describe pain differently and the pain you will tolerate will not be the same on the NRS scale. Generally speaking, it’s best not to cause the patient anything other than mild pain. According to research (2), mild pain would be up to 5/10 on the NRS scale. For example, in the acute phase of an adductor strain, if I advise the athlete to perform a core stability exercise such as dead bugs, where the injured muscle is not the main muscle in the exercise, and he/she feels pain 5/10, I will continue with the exercise. However, if the pain progresses to 6 or 7/10, I will stop and replace the exercise with another.
By combining two scales, RPE or RIR and NRS pain scale, we can get the answer to the question “How much we want to load?” In this case, the first parameter would be the pain scale we want the athlete to tolerate. Since it is normal to feel pain during rehabilitation, we would let the athlete work with pain as high as 5/10. The second parameter would be the RPE scale. Again, in this specific case, let’s give the athlete an RPE scale of 6-7. So, a 6-7/10 in RPE would mean the athlete stops the exercise approximately 3-4 reps before failure. If he experiences pain in that rep range that is higher that 5/10, he will stop the exercise immediately, never mind the RPE score. So, this will give the athlete specific instructions regarding his exercise, and we as a coach or a physio will know what range of pain and exercise effort the athlete is working in.
Repetitions in reserve (RIR)
Reps in reserve is also a subjective measure. Here, an athlete does an exercise just until they are completely worn out, and they still have enough energy for 2-3 more reps. If we take a squat with the load of 80 kg, and the maximum number of repetitions is 8, the athlete should stop at 6 reps. In the case of RIR, the lesser the value (lowest being 0), the higher the intensity. Both methods are shifting the focus from a rep, set, and weight progression to exercise effort.
So, one day the athlete could be in a great mood, strong, and painless and perform 8 reps of a squat with 80 kg on their back, while on some other day outside stressors (sleep, outside environment) might reflect badly on the athlete and they can do only 6 reps of the same exercise. On the mentioned two days, there will be different training load in regards to 1 RM, but in terms of RPE or RIR, they will be the same. So, the athlete will feel more confident and satisfied when they walk off the field because they know that the goals of the day are accomplished.
So, the athlete will feel more confident and satisfied when they walk off the field because they know that the goals of the day are accomplished.
Take home message
Every rehabilitation and RTS process is specific and we cannot operate on a cookie-cutter principle when working with injuries. However, there are similar and same diagnoses that require rehabilitation which should follow the same principles.
Do not think you can reduce anything to zero. You will have injuries, and even recurrent injuries sometimes.
Communicate openly and be specific regarding the duration of the process so that both you and the athlete have realistic expectations. Set milestones so you can check your progress and know what to expect in certain rehabilitation phases. Choose one exercise intensity measure such as RPE or RIR, it doesn’t have to be measured in kg or cm.
References:
- Serner A, Weir A, Tol JL, Thorborg K, Lanzinger S, Otten R, Hölmich P. Return to Sport After Criteria-Based Rehabilitation of Acute Adductor Injuries in Male Athletes: A Prospective Cohort Study. Orthop J Sports Med.
- Boonstra AM, Stewart RE, Köke AJ, Oosterwijk RF, Swaan JL, Schreurs KM, Schiphorst Preuper HR. Cut-Off Points for Mild, Moderate, and Severe Pain on the Numeric Rating Scale for Pain in Patients with Chronic Musculoskeletal Pain: Variability and Influence of Sex and Catastrophizing. Front Psychol. 2016 Sep 30.